Nurse Spotlight
Healthcare Documentation
Nurses Service Organization (NSO), in collaboration with CNA, has published our 4th Edition of the NSO/CNA Nurse Liability Claim Report. It includes statistical data and case scenarios from CNA claim files, as well as risk management recommendations designed to help nurses reduce their malpractice exposures and improve patient safety.
You may access the complete report, and additional Risk Control Spotlights here.
This Nurse Spotlight focuses the analysis and risk recommendations regarding one of the most significant topics in the report and for nursing professionals: Healthcare Documentation.
Nursing Allegations Related to Healthcare Documentation
While documenting care represents a critical component of nursing processes and standards, the electronic health record [EHR] has posed a level of complexity for nurses who are often challenged with why, how, what and where to document in a patient’s EHR.
Documentation deficiencies are contributing factors to many nurse professional liability claims, as well as license protection matters. However, in the 4th Edition of the NSO/CNA Nurse Liability Claim Report, failure to document or falsifying documentation closed claims, as an allegation of professional liability, increased in distribution and severity when compared to the 2011 closed claim report and the 2015 closed claim report.
To the right is an example of a professional liability claim asserted against a nurse due to the failure to document.
NURSE LEGAL CASE STUDY
Absence of documentation in violation of nursing standard of care
Comparison of 2011, 2015, 2020 Claim Reports
Average Total Incurred of Closed Professional Liability Claims by Documentation Allegations.
In the 2011 closed claim report, 0.2 percent ($31,250) of all closed claims were related to inadequate or inappropriate documentation as the primary allegation. This data increased slightly to 0.5 percent ($139,920) in the 2015 closed claim report. Respectively, in the 2020 closed claim report, documentation allegations represent 2.0 percent ($238,761) of all closed claims.
The chart demonstrates the increase in severity of professional liability claims related to documentation allegations. While these professional liability claims occur infrequently in the 2011, 2015 and 2020 closed claim analyses, allegations related to documentation failures can be difficult to defend and often result in a license protection defense matter against the nurse.
License Protection Allegations Related to Documentation Errors and Omissions
The chart displays license protection matters with defense expense payments that involve allegations related to documentation. Documentation as a primary allegation comprises 9.7 percent of all license protection matters in the Nurse Liability Claim Report: 4th Edition. Approximately half of the license protection matters related to documentation involve an allegation of fraudulent or falsified patient care or billing records (4.8 percent).
A nurse’s license is one’s livelihood, and its protection is paramount. A nurse’s practice and behavior is expected to be safe, competent, ethical and in compliance with applicable laws and rules. However, when a complaint is filed, nurses must be equipped with the resources to adequately defend themselves. Being unprepared may represent the difference between a nurse retaining or losing the license to practice, a suspension or fine.
0%
Fraudulent/falsified patient care or billing records
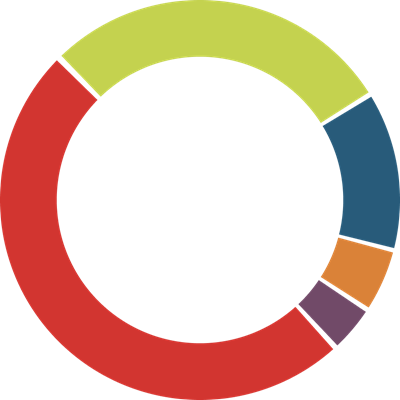
49.6%
28.6%
12.8%
5.3%
3.8%
The False Claims Act
While documentation deficiencies may result in a professional liability claim and/or a license protections matter, nurses also may be subject to federal and state sanctions for knowingly falsifying healthcare documentation under the federal False Claims Act (FCA). The FCA imposes liability on any person who submits a claim to the federal government that they know (or should have known) is false. An example may be a healthcare provider who submits a bill to Medicare for medical services they know they have not provided. The False Claims Act also imposes liability on an individual who may knowingly submit a false record in order to obtain payment from the government. For additional information on fraud and abuse laws, please see the Office of Inspector General’s provider education materials on Fraud & Abuse Laws.
Healthcare Documentation: Minimizing Risks, Maximizing Benefits
NSO/CNA is often asked about documentation risks and recommendations to minimize those risks. Nurses are certainly aware that there are patient healthcare documenting fundamentals.

The healthcare information record is a legal document that is an essential tool to:
- Document the services provided regarding the patient’s illness or injury, response to treatment, and caregiver decisions;
- Communicate documented information about the patient’s plan of care and outcomes to the health care team
- Communicate information to other nursing professionals and healthcare providers;
- Support the appropriate information for billing coding; and
- Serve as the organization’s business and legal record.
Because complete, accurate and legible healthcare records constitute an essential risk management measure, nurses should maintain proper documentation practices and follow facility policies and procedures governing appropriate and comprehensive records documentation. The facility’s healthcare record documentation policies and procedures should address, at a minimum:
- Correcting documentation errors;
- Delineating appropriate use of the copy and paste function in the electronic healthcare record;
- Documenting practices during electronic system failures or outages (“down-time”);
- Maintaining patient confidentiality
- Releasing patient healthcare information records and auditing practices; and
- Procedures for late or delayed entries


QUESTION 1/7
Documentation is only important for nurses to complete in case you get sued.

QUESTION 2/7
The State Board of Nursing can discipline nurses if their documentation needs to be revised.

CORRECT!
The answer is true.
NSO and CNA’s latest Nurse Liability Claim Report found that documentation was cited as a primary allegation in 9.7 percent of all license protection matters.
INCORRECT.
The answer is true.
NSO and CNA’s latest Nurse Liability Claim Report found that documentation was cited as a primary allegation in 9.7 percent of all license protection matters.
QUESTION 3/7
Failure to document patient care in the healthcare information record can expose a nurse to which of the following professional risks?
State Board of Nursing complaint.

QUESTION 4/7
Which of the following should not be included in the healthcare information record?

CORRECT!
The answer is: Personal opinions about the patient’s lifestyle.
Documentation in the patient healthcare information record should be objective; nurses should avoid documenting their personal opinions that are not relevant to the patient’s care. Additionally, nurses should be aware that patients have a right to access their healthcare information records.
INCORRECT.
The answer is: Personal opinions about the patient’s lifestyle.
Documentation in the patient healthcare information record should be objective; nurses should avoid documenting their personal opinions that are not relevant to the patient’s care. Additionally, nurses should be aware that patients have a right to access their healthcare information records.
QUESTION 5/7
Which of the following is not a common allegation made against nurses related to documentation?

CORRECT!
The answer is: Failure to simplify documentation.
While documentation should be concise, it is also important that documentation is complete. Documentation should accurately reflect the patient care and services provided, the patient’s response to treatment, and communication with other practitioners and the patient related to their care. Nurses should maintain proper documentation practices and follow facility policies and procedures governing appropriate and comprehensive documentation.
INCORRECT.
The answer is: Failure to simplify documentation.
While documentation should be concise, it is also important that documentation is complete. Documentation should accurately reflect the patient care and services provided, the patient’s response to treatment, and communication with other practitioners and the patient related to their care. Nurses should maintain proper documentation practices and follow facility policies and procedures governing appropriate and comprehensive documentation.
QUESTION 6/7
In case of a non-response or delayed response from a primary/consulting provider during an urgent or emergent situation, nurses should document:

CORRECT!
The answer is: All of the above.
It is advisable for nurses to document each of these steps taken to demonstrate that they acted as their patient’s advocate. Nurses are responsible for obtaining the care and services necessary for the timely treatment of patients under their care, and this responsibility continues to the point of resolution.
INCORRECT.
The answer is: All of the above.
It is advisable for nurses to document each of these steps taken to demonstrate that they acted as their patient’s advocate. Nurses are responsible for obtaining the care and services necessary for the timely treatment of patients under their care, and this responsibility continues to the point of resolution.
QUESTION 7/7
You do not need to document the use of translator services; document the patient’s care as you would any other patient.


Risk Management Recommendations: Documentation
- Clinical Content
- Medications and Prescriptions
- Diagnostic Tests, Referrals, Consultations
- Patient Education

Nursing Scope and Standards of Practice
According to the American Nurses Association (ANA), documentation represents a critical competency of all nursing processes and standards of practice (ANA Nursing Scope and Standards of Practice 3rd Edition, 2015).
The ANA Standards of Practice Competencies include the following criteria for appropriate documentation:
- Documents relevant patient data accurately and in a manner accessible to the inter-professional team (ANA Standards of Practice, Standard 1. Assessment).
- Documents the patient’s nursing and medical diagnosis, problems and issues in a manner that facilitates the determination of the expected outcomes and plan (ANA Standards of Practice, Standard 2. Diagnosis).
- Documents expected patient outcomes as measurable goals (ANA Standards of Practice, Standard 3. Outcomes Identification).
- Documents the patient’s plan of care with the prescribed strategies used to attain expected measurable outcomes using standardized language or recognized terminology (ANA Standards of Practice, Standard 4. Planning).
- Documents implementation and any modifications, including changes or omissions, of the identified plan (ANA Standards of Practice, Standard 5. Implementation).
- Documents the coordination of care (ANA Standards of
- Practice, Standard 5A. Coordination of Care).
- Documents the results of the evaluation (ANA Standards of Practice, Standard 6. Evaluation).
- Documents nursing practice in a manner that supports quality and performance improvement initiatives (ANA Standards of Practice, Standard 14. Quality of Practice).
Increase your knowledge with NSO!
Want to learn more? You can receive helpful risk management resources from NSO, including case studies, articles, checklists & much more. Sign up today! You can opt out at any time.
Nurse Spotlight

Defending Your License

Medication Administration

Liability for Nurse Managers

Depositions

Communication
